Scoliosis Neurological Exams and Chiari Malformation

Scoliosis Neurological Exams and Chiari Malformation: Scoliosis is part structural, and partly neurolgical. Scoliosis Neurological exams should be thorough and routine. A Scoliosis neurological exam should include evaluation for pathological reflexes, ankle clonus, superficial abdominal reflexes, vestibular system function, oculomotor function, brainstem and cerebellar findings.
Scoliosis neurological exams may reveal anatomical findings such as; The Chiari I malformation, also known as the Arnold-Chiari malformation, is a relatively common syndrome caused by displacement of the cerebellar tonsils below the level of the foramen magnum. Associated with the Chiari malformation may be hydrocephalus, spina bifida, and syringomyelia. In most instances, symptoms present in middle age. There are hundreds of articles about this well known malformation in the literature (see Pubmed).
Scoliosis Neurological Exams
Scoliosis progression rates can be adversely affected by neurological imbalances. Through the use of neurodiagnostic testing and structural imaging, physicians can effectively rule out known risk factors. Our doctors use EMG/NCV to test the health of the peripheral nerves as well as the nerve roots which can be irritated in the adult. VNG, EEG, and Evoke Potential testing is necessary to identify brain lateralization which can occur in early adolescents making scoliosis progression more likely.
Cause of the Chiari Malformation
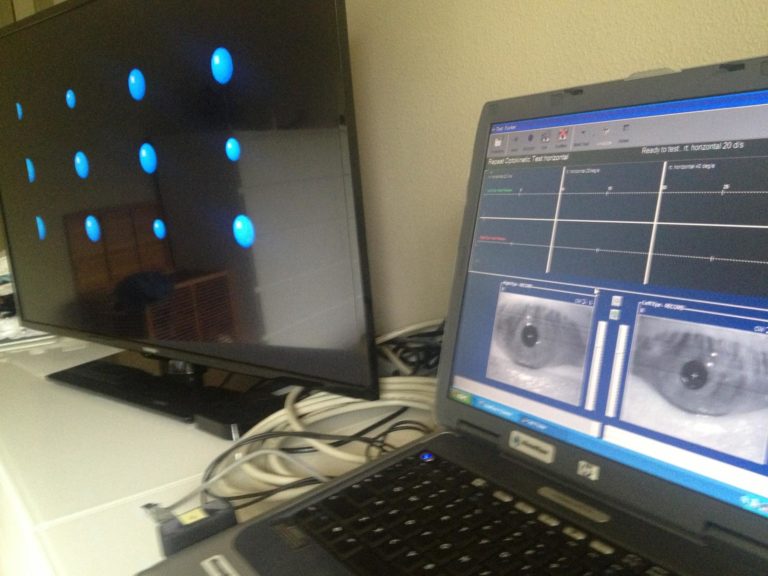
oculomotor testing

vestibular testing
Rarely there is a hole in the brainstem/spinal cord associated with the Chiari malformation (see picture below). This is called a “syrinx”. A more subtle form of this is a “presyinx”, which is a potentially reversible state of spinal cord edema caused by obstruction to normal CSF flow pathways, especially in the cervical region (Goh et al, 2008).
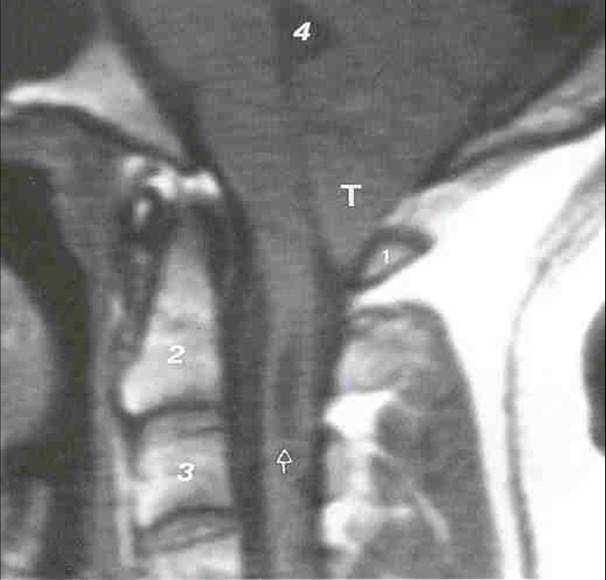
Syrinx in cervical spinal cord of individual with an Arnold Chiari Malformation. Image courtesy of Ruth Ramsey, M.D.
A closely related condition, basilar invagination may also be congenital or acquired (from arthritis).
Diagnosis of the Chiari Malformation
Often when a person presents to the office with an undiagnosed Chiari, they have dizziness and headaches. This symptom complex triggers off a set of tests for inner ear conditions. During the clinical examination or perhaps on the ENG test, downbeating nystagmus is noticed at some point, and an MRI is obtained (see above). The MRI establishes the diagnosis.

Weak downbeating nystagmus seen in primary position during ENG, in patient with a prominent Chiari Malformation. In this patient the findings on clinical examination were much more obvious than this minimal DBN seen on ENG.
Much stronger downbeating nystagmus seen on eccentric gaze, in patient with a prominent Chiari Malformation. There is no rebound nystagmus — he has a right-beating nystagmus that remains direction fixed on centering.
The definitive method of diagnosis is with a T1 MRI scan of the posterior fossa, which documents the typical downward herniation of the cerebellar tonsils. A displacement of greater than 5 mm below the foramen magnum is considered significant. Occasionally Chiari symptoms occur in persons with lessened displacement of the tonsils (Milhorat et al, 1999). We are very unenthusiastic about surgical intervention in these patients (see later comments about the difference in enthusiasm between surgeons and others).
Curiously, the author has encountered patients from time to time in which the reading radiologist did not notice that the person had a Chiari malformation. In once case, it was a very substantial one. Because of this, we think it is prudent for the doctors who notice downbeating nystagmus on examination, to review the images of their patient’s MRI’s.
Symptoms of Chiari Malformation
Symptoms suggestive of Chiari include posterior headaches, dizziness and ataxia (especially associated with straining), fainting with a cough, and weakness or numbness. A recent review of the otologic manifestations of Chiari in 16 patients indicated that 81% reported episodic aural fullness, 81% tinnitus, 69% vertigo, and 56% flutuating hearing. Headache was also common (about 80%).
Some patients with Chiari develop symptoms (dizziness mainly) on straining. This pressure sensitivity symptom is also shared by persons with superior canal dehiscence (SCD). Oddly, a recent report suggests that the Chiari Malformation is far more common in SCD (Kuhn and Clenney, 2010) than the normal population. We think that this report is likely due to sampling bias (i.e. this isn’t generally true). Nevertheless, we think it it is prudent to look for Chiari in SCD with an MRI.
Signs of Chiari Malformation
Signs of a significant Chiari malformation often include downbeat nystagmus (see above), poor pursuit for age, and alternating skew deviation.
Poor and extremely asymmetrical horizontal pursuit in person with prominent Chiari.
Poor vertical pursuit in person with prominent Chiari. Vertical pursuit is often poor in persons with no neurological disorder so the value of this is limited.
Rebound nystagmus can often be seen with a video-ENG device where the eyes can be viewed in complete darkness.
Occasionally Chiari patients will have sensorineural hearing loss (Hendrix, 1992). Positional nystagmus is common. It is most commonly downbeating or lateral beating.
Persons with Chiari may develop vertigo after spending some time with their head inclined on their trunk. Thus the Chiari can cause cervical vertigo.
In the Dix-Hallpike maneuver for BPPV, this may be recognized by seeing a delayed onset positional nystagmus. This nystagmus can also be looked for more specifically with the “vertebral artery test” — a misnomer in this particular situation.
Differential Diagnosis of downbeating nystagmus
Other causes of constant downbeating nystagmus that should generally be considered are migraine,paraneoplastic cerebellar degeneration, and anterior canal BPPV. Generally, the paraneoplastic differential is the most concerning as the nystagmus can be very strong and the consequences of missing a tumor high. Anterior canal BPPV nystagmus is not a major differential as it is present only lying flat (unlike Chiari). Migraine nystagmus is almost always weak although it is accompanied by headache like Chiari.
Chiari symptoms overlap with those of Meniere’s disease as well as migraine (Sperling et al, 2001)
RISK OF THE CHIARI
A very few individuals with the Chiari malformation develop progresive neurological symptoms. This is most commonly due to an enlarging syrinx — a hole in the spinal cord (see above). In our otoneurology practice in Chicago, it is extremely rare for us to refer patients for surgery. Rather, we generally make arrangements to follow people on a yearly basis.
In our opinion, lumbar punctures, epidural blocks and related procedures that might cause a spinal fluid leak should be avoided whenever practical in persons with known Chiari malformation. The reason to avoid these procedures is that they may worsen the Chiari.
Differential Diagnosis of downbeating nystagmus
The literature concerning treatment is large and is almost completely the work of neurosurgeons. There have been several recent review articles concerning indications for surgical treatment (Haroun, Guarnieri et al. 2000, Tubbs and Oakes 2004). There are very few articles concerning conservative management.
The following are the author’s opinions:
Neurosurgical Consultations
Decisions regarding surgery are best based on patient cost/benefit. The cost of brain surgery is substantial – medical risk, monetary cost, and time cost. The main benefit to Chiari surgery is prevention of progression of a condition that is rarely progressive.
Chiari surgery is nearly always best avoided in persons who have no neurological signs referable to the posterior fossa. In other words, don’t operate for symptoms of headache or dizziness — only operate for progressive physical signs that are unequivocally due to the Chiari.
Decisions regarding whether or not surgery is indicated are best made by non-surgeons (i.e. neurologists), as surgeons are often biased towards surgery due to their training, inclination towards active treatments, and other factors. It is safest to get a second opinion from a non-surgeon, unaffiliated with the surgeon. Ideally, ask a neurologist in a different city. An unbiased second opinion could avoid a lifetime of neurological injury.
Non-surgical Treatment
There is no medication that treats the underlying cause of the Chiari malformation (brain displacement downward). There are some medications for neck pain, headache and dizziness that may help with the symptoms.
Physical therapy and chiropractic manipulation of the neck does not help the Chiari malformation. In fact, it may make matters worse. We have no objection to massage.
Avoidance of activities that precipitates symptoms (such as straining, athletic activity requiring straining or involving forceful movements of the head on shoulders) is often useful. As examples, we would suggest that persons with Chiari malformations not lift heavy weights, or play football.
Who should take care of Chiari malformation patients ?
Neurosurgical oversight is paramount in cases with suspected brainstem malformations. Non-surgical treatment is necessary in most cases and can be effective in improving quality of life and reducing the need for surgeries.